Purchasing a water birth pool is a significant responsibility.
The decision should never be based on appearance, price or catalogue features alone.
In a maternity unit, a birth pool becomes part of the clinical environment, the cleaning regime, the hot and cold water system, and the manual-handling strategy.
Every fitting, outlet, seal, drain, hose and access point can either reduce risk or introduce unnecessary complexity.
Some features look reassuring at first glance.
A rim-mounted tap may appear convenient. A swan-neck spout may look elegant. A door may seem to make access easier. A built-in heating or recirculating system may sound technically advanced.
But in a healthcare setting, the first question should always be: does this feature make the pool safer, easier to clean and easier to manage – or does it create another risk point?
This guide explains the design features hospitals, birth centres, architects, procurement teams and maternity staff should question before specifying a water birth pool.
Why design matters in a maternity setting
Healthcare guidance is clear that infection prevention should be designed into healthcare environments from the beginning. HBN 00-09 states that a building’s design can help infection prevention and control by providing an environment that is easy to clean and maintain. [1]
That principle applies directly to water birth pools. A pool with fewer joints, fewer ledges, fewer penetrations and fewer unnecessary fittings is usually easier to clean, inspect, dry and return safely to use. By contrast, complex fittings can create small spaces where moisture, organic matter and microorganisms can remain after cleaning.
NICE recommends that baths and birthing pools are kept clean using a protocol agreed with the local microbiology department or infection-control guidance, and in accordance with the manufacturer’s guidelines. [2] A good pool design should make that requirement practical in a busy maternity unit, not difficult to achieve.

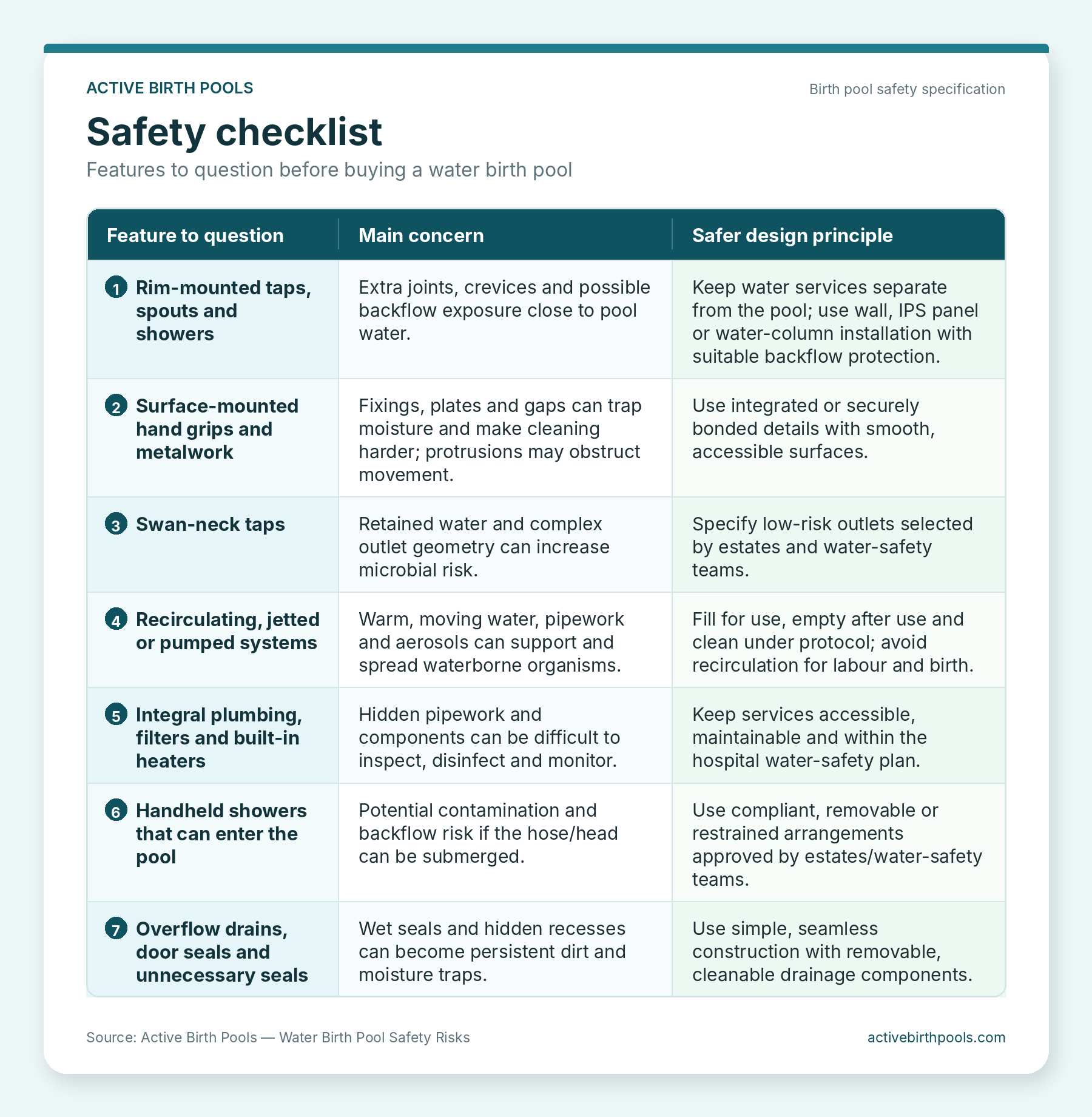
This bath shows a variety of unsafe fittings and systems that are often found on water birth pools.
Note the overflow drain, recirculating water system, swan neck tap, integral shower, rim mounted plumbing and controls.
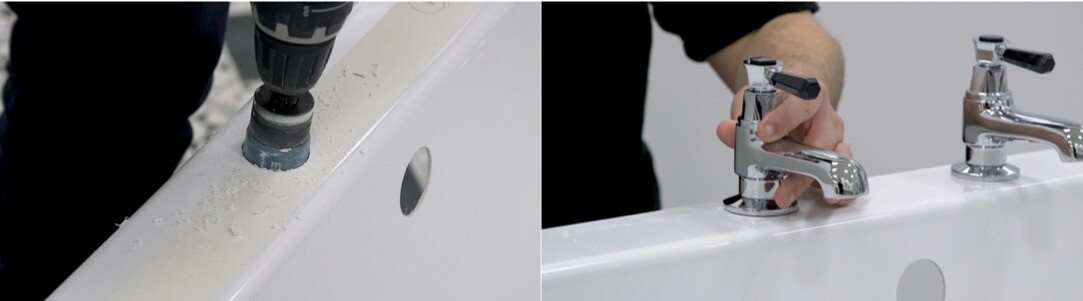
1. Rim-mounted taps, spouts and showers
Rim-mounted taps, spouts and showers should be treated with caution in a hospital water birth setting.
The issue is not only whether the fitting looks sealed. Bacteria and biofilm are microscopic. Small gaps around a base plate, tap hole, washer or fixing can retain moisture and residue. These areas can be awkward to reach during routine cleaning and inspection.
There is also a water-safety consideration. Water Regs UK notes that all bathroom water fittings need appropriate backflow protection rated to the highest downstream contamination risk, and that showers in healthcare premises can be treated as Fluid Category 5 risk. [3] In a water birth room, the estates team and water-safety group should therefore be closely involved in the specification of taps, showers, hoses, backflow protection and outlet positioning.
Safer principle: keep taps and spouts off the pool rim. Fill the pool from wall-mounted services, an IPS panel or a purpose-designed water column.
This keeps the pool simpler, leaves fewer holes and fittings in the shell, and allows water services to be managed as part of the hospital’s water system rather than as part of the pool itself.
2. Surface-mounted hand grips and internal metalwork
Handholds are important. Mothers need secure support when entering, leaving and changing position in the pool. The question is how that support is provided.
Surface-mounted hand grips, rails and metal plates can introduce fixing points, edges and narrow gaps.
If they sit inside the pool or on the rim, they may come into direct contact with pool water and can make cleaning more complicated.
They can also create protrusions that interfere with movement, comfort and midwife access.
In a clinical setting, cleanability matters as much as strength. A well-designed support feature should feel secure, be easy to wipe, avoid exposed fixings and avoid unnecessary ledges or dirt traps.
Active Birth Pools address this by using integrated, bonded hand grips designed to provide stable support while keeping the internal pool environment smooth, accessible and cleanable.

3. Swan-neck taps and retained water
Swan-neck taps may look attractive, but they are not ideal for a water birth environment.
Their shape can retain water after use, and retained water can contribute to microbial biofilm formation if outlets are not designed, flushed and maintained correctly.
HTM 04-01 gives healthcare premises guidance on the design, maintenance and operation of hot and cold water systems, including control and management of risks from Legionella, Pseudomonas aeruginosa and other waterborne pathogens. [4]
The lesson for birth-pool specification is simple: avoid decorative or domestic-style outlets where a lower-risk, healthcare-appropriate outlet would be easier to manage. Outlet choice should be made with the hospital’s estates, infection-control and water-safety teams.

4. Recirculating, jetted and pumped water systems
Recirculating systems, spa-style jets, pumped heating systems and whirlpool features have no place in a modern hospital water birth pool.
They add pipework, pumps, cavities, valves and hidden wet areas. Once microorganisms enter these systems, they can be difficult to remove. Recirculating or aerating systems can also generate aerosols when bubbles break or water is agitated, increasing the potential route of exposure.
NHS England issued a patient safety alert about heated birthing pools with built-in heaters and recirculation pumps filled in advance of labour. [5] Public Health England later reported that, after a recall of heated home birthing pools, 4 of 6 tested pools were positive for Legionella and 3 also tested positive for other potentially harmful organisms including Pseudomonas aeruginosa. [6]
This does not mean fixed hospital birthing pools are unsafe. The concern is specifically with unnecessary heating, storage, recirculation and hidden systems. The safer approach is to fill the pool for use, monitor water temperature during labour, empty the pool after use and clean it under local protocol and manufacturer guidance.
5. Integral plumbing and hidden services
Integral plumbing systems can look neat, but hidden pipework is rarely an advantage in a healthcare environment.
Flexible hoses, internal pipes, pumps, filters, valves, heaters and concealed spaces can be difficult to inspect, disinfect, maintain and monitor.
Stagnant water in dead legs or rarely used sections of pipework is a recognised water-safety concern. The HSE notes that hot and cold water systems can present a foreseeable risk of exposure to Legionella, and that understanding the water system and its parts – including dead legs, TMVs and outlets – is necessary for risk assessment. [7]
For hospitals, the safer design principle is separation. The birth pool should be a fixed, cleanable sanitary-ware product. The water services should be specified, installed, accessed and maintained by the hospital’s estates team as part of the wider water-safety plan.
6. Handheld showers and hose management
Handheld showers are a common source of confusion. They are useful for cleaning the pool after use, but they can create a risk if the hose or handset can enter the pool water during use.
Water Regs UK explains that shower installations must have appropriate backflow protection and that, in high-risk settings such as healthcare premises, showers may be classed as Fluid Category 5 risk. Hose handsets capable of reaching contaminated water sources require suitable Fluid Category 5 backflow-prevention arrangements unless the hose is permanently restrained or shortened to maintain an adequate gap. [3]
For water birth rooms, the safe approach is to prevent the shower hose or head from entering the pool during labour and birth, and to ensure the design is approved by estates and the water-safety group.
A removable cleaning hose may be acceptable where it is detached when the pool is in use and used only after the pool has been emptied for cleaning, subject to local approval.

7. Built-in filters and disinfection devices
Filters and disinfection devices should not be used to justify a poor basic design.
If a pool relies on filters to compensate for built-in plumbing, recirculation, hidden pipework or complex wet components, the underlying problem remains. Filters require maintenance, monitoring and replacement. They can reduce risk only when they are correctly specified and managed within a formal water-safety system.
The better design principle is to remove avoidable risk at source: no recirculation, no hidden wet systems, no unnecessary pipework inside the pool and no complex internal fittings that are difficult to access.
8. Overflow drains and hidden wet recesses
Overflow drains are another feature borrowed from baths and spa products that should be questioned in water birth pools.
An overflow adds hidden surfaces, internal channels and wet recesses.
These areas can be difficult to access during routine cleaning and can retain moisture between uses. If a feature cannot be reliably cleaned, inspected and dried, it should not be built into a healthcare birth pool unless there is a clear, justified reason.
The safer design principle is a simple, purpose-designed drainage system with components that can be removed, cleaned, disinfected, rinsed, dried and checked in accordance with local policy.
9. Doors, seals and access panels
A door in a water birth pool may appear helpful, but it introduces a major design compromise.
Doors require seals, hinges, locking mechanisms and joints. These features are exposed to warm water, organic matter and repeated cleaning chemicals. Any seal or hinge line can become a moisture trap.
In an emergency, a door may also complicate rather than simplify evacuation, because staff still need space, technique, equipment and coordinated manual handling.
Access should be solved through the pool’s height, internal shape, external step, handholds, midwife access and local emergency procedures – not by introducing a door and seal into the pool shell.

10. Domestic styling in a clinical environment
A maternity pool should not be specified as though it were a domestic bath, spa bath or wellness product.
In hospitals, design priorities are different. The pool must support infection prevention, water-safety governance, manual handling, cleaning, inspection, maintenance and repeated clinical use. A domestic-style feature may look reassuring in a brochure while creating avoidable work for maternity, cleaning and estates teams.
When assessing a pool, procurement teams should ask: Can every surface be reached? Can every component be inspected? Can the pool be cleaned quickly and consistently between births? Are water outlets separate and maintainable? Are there any hidden wet areas? Does each fitting justify its risk?
What safer birth-pool design looks like
A safer water birth pool is not over-engineered. It is simple, strong, cleanable and purpose-designed for maternity use.
Active Birth Pools are designed around this principle. They use smooth Ficore® surfaces, seamless one-piece construction, integrated hand grips, minimal fittings, purpose-designed drainage and water services kept separate from the pool rim. Freestanding installations can be supported by a dedicated water column so that taps, spout, shower and support rail remain separate from the pool itself.
This approach supports the same aim described in healthcare guidance: make the environment easier to clean, easier to maintain and easier to manage safely.

Buyer questions before specifying a water birth pool
Before purchasing a water birth pool, ask the supplier:
- Are there any taps, spouts, showers or controls mounted on the pool rim?
- Are any hand grips, rails or metal fittings bolted onto the internal surface?
- Does the pool include any recirculation, jets, pumps, heaters or hidden pipework?
- Can every wet surface be cleaned, disinfected, rinsed, dried and inspected?
- Are there any overflows, doors, seals or inaccessible cavities?
- Is the pool filled for use and emptied after use, rather than maintained warm in advance?
- Has the installation been reviewed by estates, infection-control and water-safety teams?
- Does the manufacturer provide clear cleaning and care guidance?
Conclusion: remove avoidable risk at source
No product can replace local clinical judgement, infection-control procedures, estates management or water-safety governance.
But good design can make those responsibilities easier to fulfil.
A hospital water birth pool should not be a spa product adapted for maternity use. It should be a fixed, purpose-designed sanitary-ware product that supports safe water use, effective cleaning, practical midwifery and maternal movement.
The safest features are often the ones that are not there: no rim-mounted taps, no jets, no recirculation, no hidden plumbing, no overflows, no doors and no unnecessary surface-mounted metalwork.
In maternity environments, simplicity is not basic. Simplicity is safer.
Evidence and source notes
[1] NHS England, Health Building Note 00-09: Infection control in the built environment. Summary states that building design can help infection prevention and control by providing an environment that is easy to clean and maintain, and that these features should be designed into a project from the beginning. https://www.england.nhs.uk/publication/infection-control-in-the-built-environment-hbn-00-09/
[2] NICE NG235, Intrapartum care recommendations. NICE recommends offering labour in water for pain relief, monitoring maternal and water temperature hourly, keeping water at or below 37.5°C, and keeping baths and birthing pools clean using agreed infection-control/microbiology protocols and manufacturer guidance. https://www.nice.org.uk/guidance/ng235/chapter/Recommendations
[3] Water Regs UK, What backflow protection is required for a shower? Water fittings in bathrooms require backflow protection appropriate to the highest downstream fluid-category risk; showers in healthcare premises can be Fluid Category 5 risk, and hose handsets require suitable arrangements if they can reach contaminated water sources. https://www.waterregsuk.co.uk/topics/all-faqs/showers/
[4] NHS England, HTM 04-01: Safe water in healthcare premises. Guidance covers legal requirements, design applications, maintenance and operation of hot and cold water supply, storage and distribution systems in healthcare premises, including the control and management of Legionella, Pseudomonas aeruginosa and other waterborne pathogens. https://www.england.nhs.uk/publication/safe-water-in-healthcare-premises-htm-04-01/
[5] NHS England, Patient safety alert: Legionella and heated birthing pools filled in advance of labour in home settings. The alert advised against birthing pools with built-in heaters and recirculation pumps potentially filled in advance of birth. https://www.england.nhs.uk/publication/patient-safety-alert-legionella-and-heated-birthing-pools-filled-in-advance-of-labour-in-home-settings/
[6] Public Health England, Legionella contamination found in more heated birthing pools. PHE reported positive Legionella results in recalled heated birthing pools and reinforced advice against heated, recirculating home birthing pools filled in advance of labour. https://www.gov.uk/government/news/legionella-contamination-found-in-more-heated-birthing-pools
[7] HSE, Hot and cold water systems. HSE notes that hot and cold water systems can present foreseeable risk of exposure to Legionella, and highlights the importance of understanding system components including dead legs, TMVs and outlets. https://www.hse.gov.uk/legionnaires/hot-and-cold.htm
[8] Original Active Birth Pools source page used as the basis for the rewrite: Health and Safety risks you need to be aware of before buying a water birth pool. https://activebirthpools.com/health-and-safety-risks-you-need-to-be-aware-of-before-buying-a-water-birth-pool/
[9] Related Active Birth Pools page used to align house style and avoid duplication: Designed to Optimise Safety, Reduce Risk and Support Safer Birthing Environments. https://activebirthpools.com/birth-pool-safety-design/


































 Conclusion
Conclusion
 A practical working surface for midwives
A practical working surface for midwives