How to Choose a Hospital Water Birth Pool: Safety, Ergonomics, Hygiene and Long-Term Value
Choosing a water birth pool is not simply a question of size or price.
For hospitals and maternity units, the right pool must support mothers, protect midwives, meet infection control expectations and deliver reliable performance for decades.
Purchasing a water birth pool is an important decision for any hospital, birth centre or maternity unit.
A pool is not just a piece of equipment placed in a room.
It becomes part of the birth environment, part of the working space for midwives and part of a mother’s experience of labour and birth.
For that reason, value should mean more than initial purchase cost.
A well-designed hospital birth pool should deliver safety, comfort, hygiene, durability and ease of use every day, year after year.
Active Birth Pools have been developed over almost four decades to meet these needs.
Every curve, surface and feature is shaped around the practical realities of maternity care: how mothers move in labour, how midwives provide support, how rooms are cleaned, how emergencies are managed and how hospitals achieve long-term value from their investment.

Why Ergonomic Design Matters
Good ergonomic design is not decorative.
It is the art of making something work beautifully for the people who use it.
In a maternity setting, this means supporting two groups at once: the mother in labour and the midwives caring for her.
A birth pool must allow mothers to move freely, rest comfortably, enter and leave safely, and adopt natural upright positions.
At the same time, it must allow midwives to remain close, work in balanced postures and respond quickly without excessive bending, twisting or reaching.
Active Birth Pools are designed around these movements.
Their flowing, organic forms are not arbitrary.
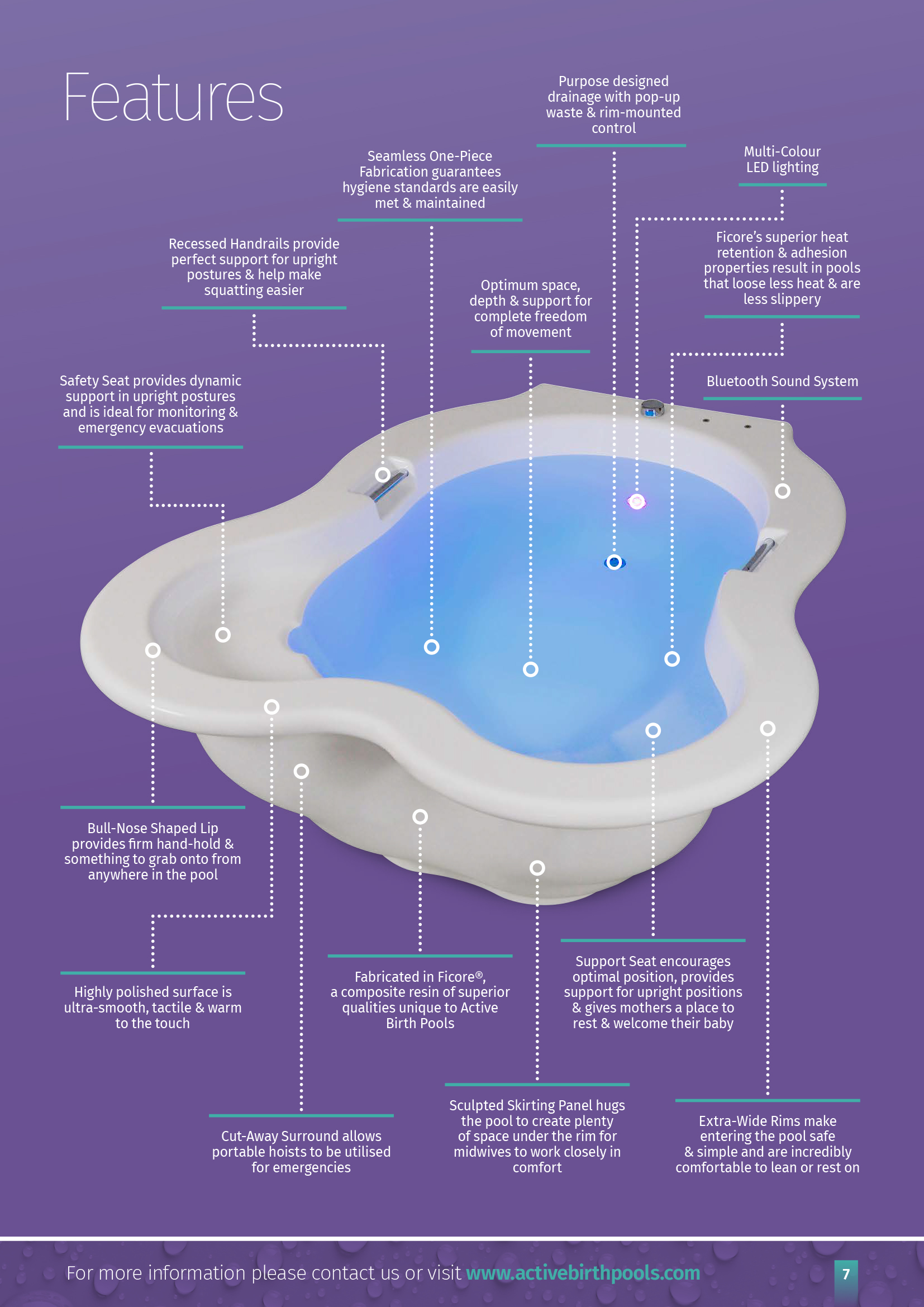
The wide rounded rims, contoured profiles, integrated seating and recessed handgrips all serve a purpose.
They help mothers feel secure and supported, while giving midwives better access and reducing physical strain.
The result is a pool that feels intuitive to use.
Mothers can lean, kneel, sit, squat or rest as labour progresses.
Midwives can remain close without being forced into awkward or unsafe positions.

Protecting Midwives from Strain and Injury
Manual handling is a serious consideration in maternity care.
Supporting women in labour can place midwives under significant physical strain, especially when access is restricted or when they must work over hard, narrow or obstructed pool edges.
Active Birth Pools are designed to reduce these risks.
The extra-wide wraparound rim allows midwives to rest their forearms comfortably and maintain stable positions during prolonged care.
The pool’s contours allow closer access while reducing the need to bend, twist or overreach.
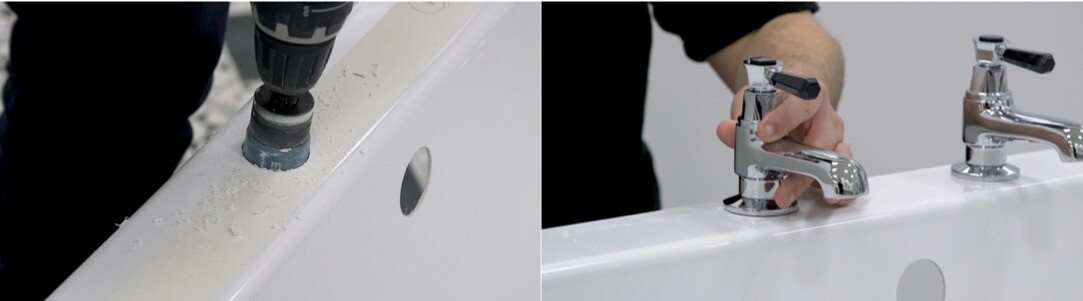
Unlike conventional designs with rim-mounted taps, fittings or protruding fixtures, Active Birth Pools keep the rim clear.
This gives midwives freedom to move around the pool and respond to the changing needs of labour and birth.
This is not only more comfortable.
It is safer, more efficient and more supportive of good clinical practice.

Helping Mothers Move Naturally in Labour
Water birth is closely associated with freedom of movement, relaxation and instinctive positioning.
Once immersed, the buoyancy of the water supports the mother’s weight, eases pressure and helps her relax more deeply.
A well-designed pool should enhance these benefits.
The interior must be spacious enough for movement, but supportive enough to feel safe.
It should encourage upright and forward-leaning positions, while allowing the mother to rest when needed.
Active Birth Pools are designed to create a calm, womb-like space where women can respond to their body’s cues.
The gently sculpted interior supports kneeling, squatting, leaning and resting.
his freedom of movement helps mothers find the positions that feel most comfortable and effective during labour.
Every detail exists to support the physiological process of labour while giving mothers a greater sense of safety, privacy and control.

Safe Entry: The “Sit and Swivel” Method
One of the most important, and often underestimated, aspects of water birth pool design is how the mother gets into the pool.
In strong labour, climbing up steps, stepping over a high rim and lowering into water can be difficult and risky.
It can also require unnecessary physical assistance from midwives.
Active Birth Pools solve this with a simple “sit and swivel” method.
The mother steps onto a single low step, sits on the extra-wide rim, swivels her legs into the pool and gently lowers herself into the water.
This allows her to maintain three points of contact and remain grounded throughout the movement.
The step unit lowers the effective height of the rim to around that of a standard bath, making access feel familiar and manageable.
It is also easy to move and does not obstruct access around the pool when not in use.
This simple approach reduces risk for mothers and helps protect midwives from the strain of physically assisting women into the pool.

Hygiene and Infection Control by Design
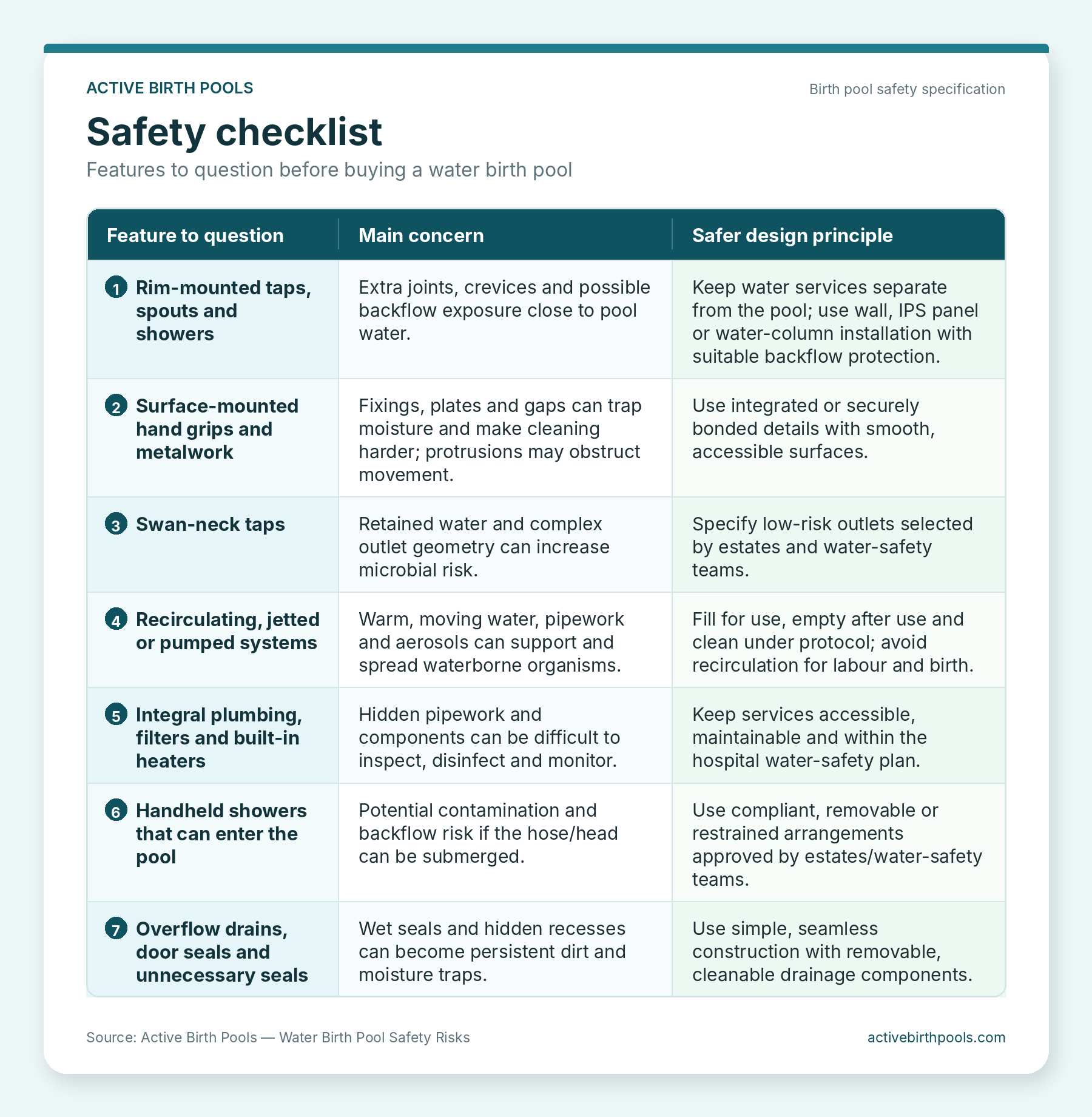
Water safety and hygiene are central to hospital birth pool selection.
Pools must be easy to clean, resistant to damage and designed to minimise the risk of bacteria accumulating in seams, joints or hidden crevices.
Active Birth Pools are made from Ficore®, a solid chemically fused composite resin developed exclusively for these pools.
Unlike acrylic or fibreglass laminates, Ficore® forms a seamless one-piece shell with a smooth, non-porous surface.
This construction helps eliminate joins, dirt traps and areas where biofilm could accumulate. The organic contours allow water to drain effectively and make cleaning quicker and more thorough.
Ficore® is also more slip resistant and less slippery than fibreglass or acrylic, while providing exceptional strength, durability and a refined finish suitable for demanding clinical environments.
The absence of unnecessary surface-mounted metalwork further supports infection control.
Recessed stainless steel handgrips are fully bonded into the structure rather than bolted or rim-mounted, helping to reduce cleaning and maintenance concerns.

Emergency Evacuation
Although emergency evacuation from a birth pool is rare, every maternity unit must have clear protocols in place.
Active Birth Pools are designed to make this process safer and simpler.
Extra-wide rims and integrated support seats help staff move the mother into a secure position before transfer.
Because the rim is clear of obstructing taps and fittings, access is less restricted.
The mother can be gently moved onto the internal seat, supported safely while additional staff and a trolley are brought into position, then transferred over the wide, softly contoured rim.
Active Birth Pools are also compatible with portable hoists.
Unobstructed access under and around the rim allows a hoist to be brought into position when required, offering an additional layer of safety and flexibility.

Why Ficore® Composite Makes the Difference
The material used to manufacture a hospital birth pool has a direct impact on strength, hygiene, comfort, durability and long-term value.
Ficore® composite allows Active Birth Pools to be manufactured as seamless, one-piece structures with exceptional structural integrity.
It enables refined curves, smooth radii and an organic form that would be difficult to achieve with conventional materials.
Ficore® also helps retain heat, resists hospital-grade cleaning chemicals and maintains its finish despite continuous use.
Because the pools are built to last for decades and require minimal maintenance, they offer strong lifecycle value for hospitals and birth centres.
For maternity units under pressure to deliver more with less, this matters.
A lower initial purchase price can quickly become expensive if a pool requires frequent repairs, replacement, specialist maintenance or presents ongoing cleaning challenges.
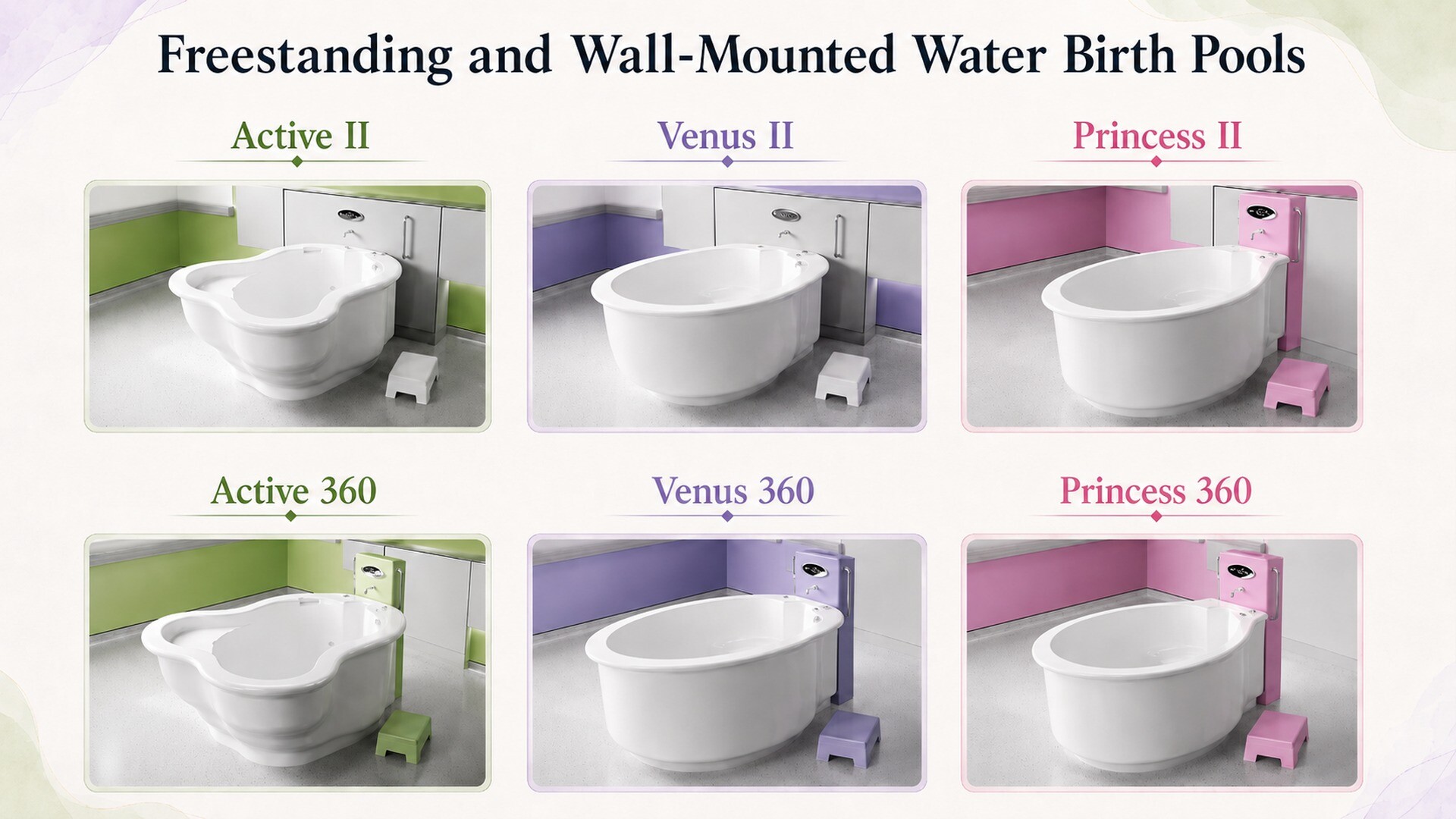 Active Birth Pools are available in three main sizes: the compact Princess, the mid-size Venus and the large Active Birth Pool.
Active Birth Pools are available in three main sizes: the compact Princess, the mid-size Venus and the large Active Birth Pool.
The right choice depends on room size, intended use and the level of access required around the pool.
As a general principle, hospitals should choose the largest pool that comfortably fits the room, while leaving sufficient working space around it.
A minimum of around 80 cm is recommended at the sides, with 150–200 cm in front of the pool wherever possible.
Wall-mounted pools provide excellent access while saving space and reducing installation costs.
Freestanding 360° models allow movement all the way around the pool and use a specially designed Water Column to house plumbing and fittings away from the rim.
Options: Bespoke Water Column, Single Step Unit, Multi-Colour LED Lighting and Bluetooth Sound
For freestanding 360° pools, the bespoke Water Column provides a practical and hygienic solution for plumbing and fittings.
By removing taps and fixtures from the pool rim, it improves access, supports infection control and reduces manual handling risks.
The custom step unit supports the “sit and swivel” method of pool entry, giving mothers the height advantage they need while avoiding the risks associated with bulky multi-step units.
Optional multi-colour Chromotherapy LED lighting and Bluetooth sound can also help create a calm birth environment.
Soft ambient lighting improves visibility for midwives while helping mothers relax, and integrated sound allows music to become part of the atmosphere of the room.

Long-Term Value for Hospitals
A hospital water birth pool should be judged by its performance over time.
The best pools reduce risk, support safe practice, improve the experience of mothers and midwives, and remain reliable for decades.
They should be easy to clean, simple to maintain, comfortable to use and robust enough for demanding maternity environments.
Active Birth Pools combine ergonomic design, Ficore® composite material and bespoke manufacturing to deliver safety, hygiene, durability and long-term value.
They are designed not only to look beautiful, but to work beautifully in real clinical settings.
For hospitals, maternity units and healthcare planners, choosing the right water birth pool is a strategic decision.
It affects the quality of care, the working conditions of midwives, the experience of mothers and the long-term performance of the birth environment.

Compare whole-life value, not simply purchase price
The lowest initial quotation is not necessarily the lowest-cost option over the life of a maternity unit.
A hospital should consider expected service life, warranty, cleaning time, maintenance, repairability, reliability, energy and water use, replacement frequency, staff usability and the availability of technical support. [21,22]
Active Birth Pools states that Ficore® pools are engineered to last for decades and are guaranteed for life.
A long service life can reduce the financial and environmental cost associated with repeated replacement, while a durable and repairable surface can help maintain the pool’s performance and appearance.
A water birth pool should support the natural physiology of labour while meeting the practical demands of modern maternity care.
That requires more than a simple tub of water.
It requires thoughtful ergonomic design, advanced materials, safe access, effective infection control, emergency planning and long-term durability.
Active Birth Pools have been developed to bring these elements together in one integrated solution: safe for mothers, supportive for midwives, hygienic for hospitals and built to last.
















 Conclusion
Conclusion